Why is it useful to use our APP VIDA?
- SELECTIVE SCREENING: Increase the effectiveness of screening.
- COST REDUCCION: detecting on early time the high-risk patients will economize cost of treatments.
- SAVE LIVES: Worldwide statistics show that more than 75% of patients never do screening or do it when is too late.

TECHNICAL ASPECT OF OUR WORK
The following paper is the most complete recompilation of thermography we have found
Infrared imaging technology for breast cancer detection – Current status, protocols and new directions
Early and accurate detection of breast cancer is a critical part of the strategy to reduce the morbidity and mortality associated with this common disease. While current guidelines recommend mammography for screening, the sensitivity and specificity of mammograms remains less than optimal, especially for patients with dense breast tissue. Thermography has been explored in the past as an alternative to mammography. Advances in IR cameras that are used to obtain thermal images of the breast as well as computational tools used to accurately model heat transfer within the breast have significantly increased the accuracy of thermography. The current work reviews the progress that has been made in using thermal imaging to detect breast cancer over the past three decades and identifies aspects that need further refinement for it to become a reliable tool to diagnose breast cancer. Recent advances and suggestions for future work in the field including using advanced simulation methods, inverse modeling, imaging protocols, and using artificial neural networks to better predict the location of the tumor are also presented.
Satish G. Kandlikar a,⇑ , Isaac Perez-Raya a , Pruthvik A. Raghupathi a , Jose-Luis Gonzalez-Hernandez a , Donnette Dabydeen b , Lori Medeiros c , Pradyumna Phatak d aDepartment of Mechanical Engineering, Rochester Institute of Technology, 76 Lomb Memorial Drive, Rochester, NY 14623, USA bDepartment of Radiology, Rochester General Hospital Regional, 1425 Portland Avenue, Rochester, NY 14621, USA c Rochester General Breast Center, Rochester, 1425 Portland Avenue, Rochester, NY 14621, USA dDepartment of Medicine and Lipson Cancer Institute, Rochester General Hospital, 1425 Portland Avenue, Rochester, NY 14621, USA.
Article history: Received 8 November 2016 Received in revised form 17 January 2017 Accepted 21 January 2017 Available online 6 February 2017.
Design of vein finder with multi tuning wavelength using RGB LED
The light characteristic on skin The skin can be penetrated by light at specific wavelengths. The light is divided into three criteria in the breakout. Three criteria in the light of which light with a wavelength of 200-400 nm can only penetrate the epidermis skin layer, light with a wavelength of 400-600 nm can penetrate the dermis layer of the skin, whereas light with a wavelengths of 600-700 nm can penetrate the skin subcutaneous tissue (Figure 1). Properties of the skin fired with the light reflect, scatter and absorb it. Figure 1. Wavelength of Light to Penetrate Skin [4] When the wavelength of visible light is 400-700 nm fired onto skin then some light will be absorbed, reflected and diffused into other parts of the skin. If the light wavelength range of 400-600 nm value then the light is merely distributed on the dermis only, whereas if the light wavelength of 600-700 nm, the light will spread and reach the subcutaneous layer of the skin in which there are blood vessels. Absorption, reflection and light transmission were fired can be seen in Figure 2. Colours absorbed by the skin will be forwarded to the subcutaneous layer where a vein is located. Vena will look black on the surface of the skin when exposed to light at these wavelengths. This is because haemoglobin in the blood absorbs the light so that the veins will be looks dark.
Franky Chandra1*, Aries Wahyudianto1 , and M Yasin2 1 Biomedical Engineering, Faculty of Science and Technology, Airlangga University, Surabaya (60115), Indonesia 2 Physics, Faculty of Science and Technology, Airlangga University, Surabaya (60115), Indonesia
International Conference on Physical Instrumentation and Advanced Materials IOP Publishing IOP Conf. Series: Journal of Physics: Conf. Series 853 (2017) 012019 doi :10.1088/1742-6596/853/1/012019.

Modern smart phones are sensible to a very large wavelength spectrum as shows following image

We use their sensibility to detect angiogenic process
Even if the most of angiogenic process detected by our algorithm are placer at 10 mm depth or less, we have experimentally proved that our algorithm allows us to detect angiogenic process placed at deeper level than 10mm( publication will realized after patenting process), the physical reason of this results is thermal modulation, the hit of deeper vascular process is perceived on at 8 mm as tinny source of hit ( as a thermal shadow).
Our results

On the left image if is veins are clearly visible, the black dots are normal vascularization process, on the right side anormal vascularization process feeding a cancer HER-2.
Example of angiogenic process , left side normal , right side pathologic

Clinical Procedure
For patient at home, using only Vida app
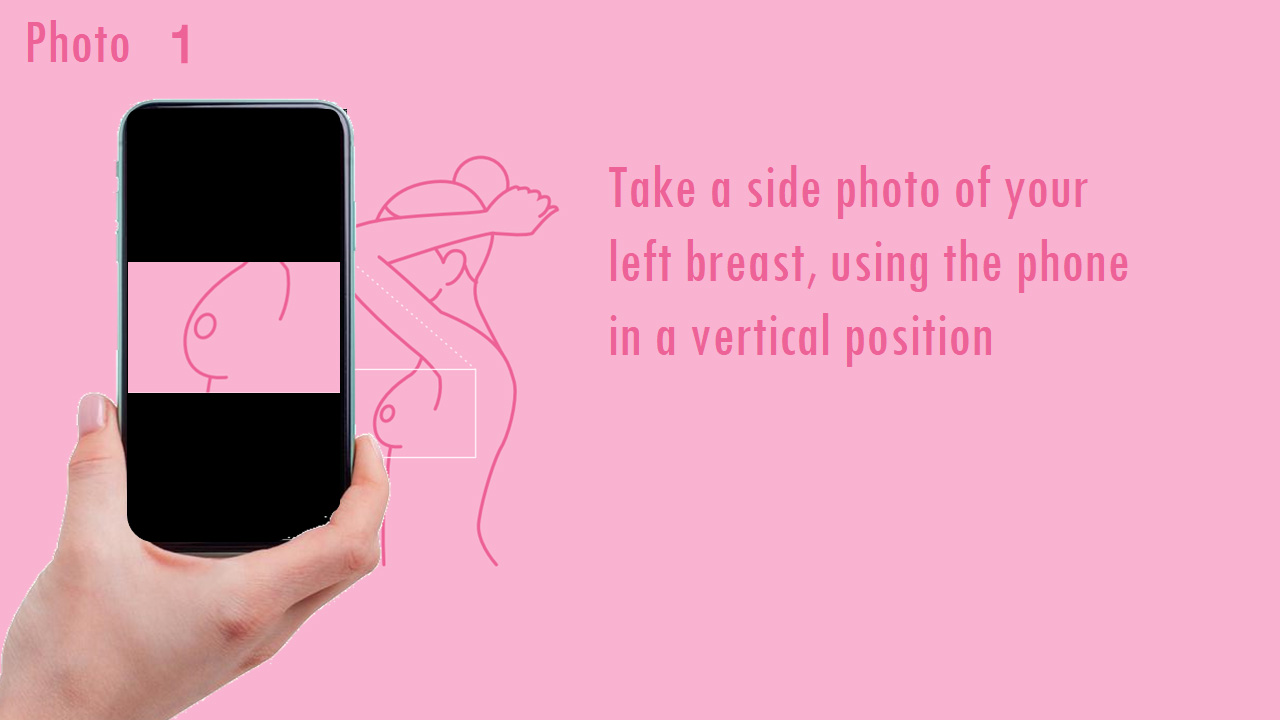
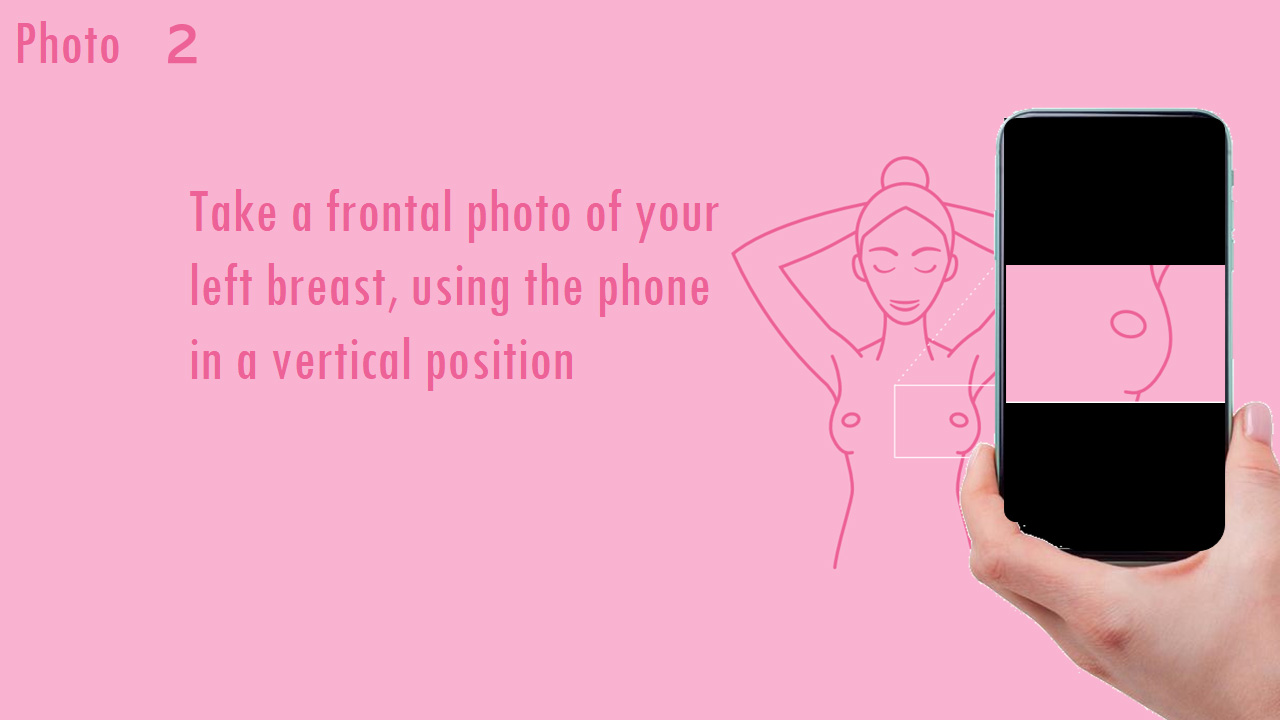
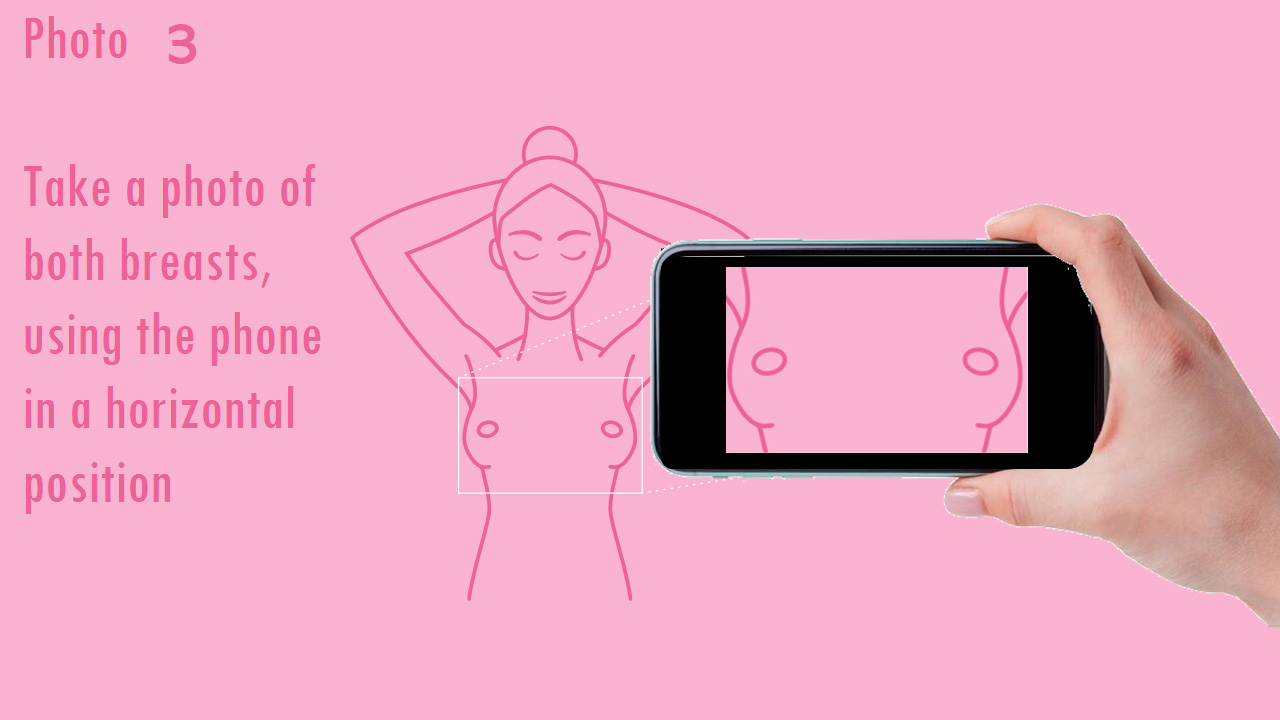
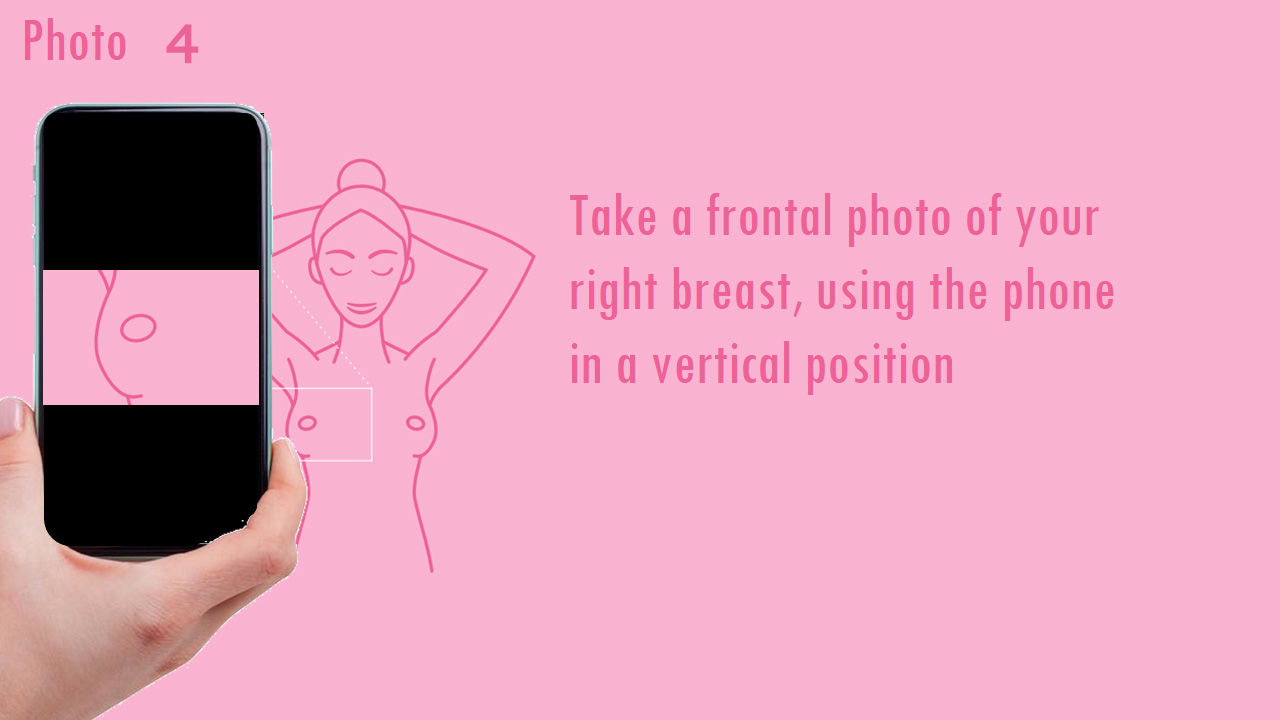
They take a sequence of photos as described on following images
Few minutes after take the pictures the patient can see on his screen, the picture from left if no vascular anomalies were detected or the right side of the image if anomalies were detected, in this last case the patient will receive a recommendation to assist to an specialist and will be informed about the importance of regular screening in function of age or familiar antecedents.


If you are a Practician
Screening using VIDA medical prototype

Protocol and procedure
- Woman without a bra, rings or necklaces/pendants.
- Approximate brightness between 150 and 300 LUX near the patient’s chest.
- Distance between the center of the tripod and the patient: 1.5 meters.
- iPad 9lights on:
- Light A set to 2500 KLight
- Light B set to RGB with R values at 255, G at 100, and B at 0
- iPad height: adjust the height to the patient’s breasts.
- Adjust zoom of the iPad between 2.8X and 3X until framing the breasts.
- First image: both breasts front view.
- Adjust zoom of the iPad between 4.5X and 5X until framing the breasts.
- Second image: left chest, front view.
- Third image: left chest, left view (patient turned 90° to the right from facing the iPad).
- Fourth image: right chest, front view.
- Fifth image: right chest, right view (patient turned 90° to the left from facing the iPad).





What will see the doctor on his practice
The doctor will have access to a large number of analysis and tools in other to have an screening results as rich as possible.

To learn more...
Several data support a central role for angiogenesis in breast cancer growth and metastasis. Observational studies have demonstrated that microvascular density (MVD) is a prognostic factor in invasive breast cancer. Vascular endothelial growth factor is the most important angiogenic factor with proven significance in breast cancer, as it has been assessed in both experimental and clinical studies.
Triple-negative breast cancer (TNBC) is a type of breast cancer which lacks estrogen, progesterone, and HER-2/neu receptors. MVD in both basal-like and TNBC is significantly higher than in non–basal-like and non-TNBC.
Translational Oncology (2016) 9, 453–457
Angiogenesis and Antiangiogenesis in Triple-Negative Breast cancer1 Domenico Ribatti*, † , Beatrice Nico* , Simona Ruggieri* , Roberto Tamma* , Giovanni Simone‡ and Anita Mangia§ * Department of Basic Medical Sciences, Neurosciences and Sensory Organs, University of Bari Medical School, Bari, Italy; † IRCCS Istituto Tumori “Giovanni Paolo II,” Bari, Italy; ‡ Pathology Department, IRCCS Istituto Tumori “Giovanni Paolo II,” Bari, Italy; § Functional Biomorphology Laboratory, IRCCS Istituto Tumori “Giovanni Paolo II,” Bari, Italy.
Mean microvessel densities (MVD) were determined by counting von Willebrand factor stained cells in three separate “vascular hot spots” using image analysis. Tumor samples were also stained for HER-2 by IHC, HER-2 gene amplification by fluorescence in situ hybridization, carbonic anhydrase 9 by IHC, and vascular endothelial growth factor (VEGF) by IHC. Plasma from 36 patients with primary tumor samples had VEGF (R&D Systems, MN) and D-dimer (American Diagnostica, Greenwich, CT) levels determined. Results: There was a significant positive correlation between HER-2 gene amplification and both maximum and average MVD (Spearman coefficient 0.51 and 0.50; P 0.03 and 0.05, respectively).
HER-2-amplified breast cancers have increased amounts of angiogenesis, decreased amounts of hypoxia, and increased markers of fibrin degradation. These findings have prognostic, predictive, and therapeutic implications in breast cancer treatment.
Vol. 10, 4083–4088, June 15, 2004 Clinical Cancer Research 4083
Kimberly L. Blackwell,1 Mark W. Dewhirst,1 Vlayka Liotcheva,1 Stacey Snyder,1 Gloria Broadwater,1 Rex Bentley,1 Anita Lal,3 Gregory Riggins,1 Steve Anderson,2 Jim Vredenburgh,1 Alan Proia,1 and Lyndsay N. Harris4 1 Duke University Comprehensive Cancer Center, Durham, North Carolina; 2 Labcorp Inc., Research Triangle Park, North Carolina; 3 Brain Tumor Research Center, Department of Neurological Surgery, University of California San Francisco, San Francisco, California; and 4 Dana-Farber Cancer Institute, Boston, Massachusetts.
Angiogenesis is an essential step for breast cancer progression and dissemination. The development of new blood vessels in cancer setting (angiogenesis) is conducted by numerous physiological and pathological stimuli, where the main stimulus is hypoxia. The knowledge of different molecular pathways regulating angiogenesis is constantly growing. An increased and complex scenario of angiogenesis is nowadays available in breast cancer, specifically, and permits not only to understand most of the important phases of neoplastic growth but also offer an exciting perspective for new therapeutic proposals based on blocking new blood vessels sprouting.
Hindawi Publishing Corporation Journal of Oncology Volume 2010, Article ID 576384, 7 pages doi:10.1155/2010/576384
Article Angiogenesis and Breast Cancer Adhemar Longatto Filho,1, 2 Jose Manuel Lopes, ´ 3, 4 and Fernando C. Schmitt3, 4 1 Laboratory of Medical Investigation (LIM), School of Medicine, University of Sao Paulo, 01246-903 S ˜ ao Paulo-SP, Brazil ˜ 2 School of Health Sciences, Life and Health Sciences Research Institute, University of Minho, Campos of Gualtar, 4710-057 Braga, Portugal 3 Institute of Molecular Pathology and Immunology, University of Porto, IPATIMUP, Rua Roberto Frias s/n, 4200 Porto, Portugal 4Medical Faculty, Porto University, 4099-002 Porto, Portugal Correspondence should be addressed to Fernando C. Schmitt, [email protected] Received 12 April 2010; Revised 29 July 2010; Accepted 2 September 2010.
CLINICAL EVIDENCE OF ANGIOGENESIS IN BREAST CANCER Clinicopathologic correlations also confirm the central role of angiogenesis in breast cancer progression. Fibrocystic lesions with the highest vascular density are associated with a greater risk of breast cancer.10 Microvessel density (MVD) was shown to be highest with histopathologically aggressive ductal carcinoma-in-situ lesions11 and associated with increased VEGF expression.12 High MVD in premalignant lesions have been associated with high risk of future breast cancer.10 Also, high MVD in invasive disease has been correlated with a greater likelihood of metastatic VOLUME 23 d NUMBER 8 d MARCH 10 2005 JOURNAL OF CLINICAL ONCOLOGY REVIEW ARTICLE 1782 Downloaded from ascopubs.org by 87.144.16.71 on September 23, 2021 from 087.144.016.071 Copyright © 2021 American Society of Clinical Oncology. All rights reserved. disease13 and a shorter relapse-free and overall survival in patients with node-negative breast cancer.14.
Bryan P. Schneider and Kathy D. Miller From the Division of HematologyOncology, Indiana University, Indianapolis, IN. Submitted December 22, 2004; accepted December 30, 2004. Supported in part by the Breast Cancer Research Foundation (K.D.M.). Authors’ disclosures of potential conflicts of interest are found at the end of this article. Address reprint requests to Bryan P. Schneider, MD, Division of HematologyOncology, Indiana University, 535 Barnhill Dr, RT-473 Indianapolis, IN 46202; e-mail: [email protected]. 2005 by American Society of Clinical Oncology 0732-183X/05/2308-1782/$20.00 DOI: 10.1200/JCO.2005.12.017 J Clin Oncol 23:1782-1790. 2005 by American Society of Clinical Oncology.
For women between the ages of 40 and 49 years undergoing annual screening mammography, CISNET modeling results estimate an NNS of 746, 39% of the NNI of 1904 estimated by USPSTF on the basis of randomized controlled trial (RCT) data. The NNS based on CISNET results for women between 50 and 59 years is 351 (26% of the NNI of 1339 estimated by USPSTF from RCT data), for women between 60 and 69 years is 233 (62% of the NNI of 377 estimated by USPSTF from RCT data), and for women between 70 and 79 years is 377. Annual screening of women between 40 and 84 years yields an NNS of 84 and an NNS/LYG of 5.3. Biennial screening of women ages 50–74 yields an NNS of 144 and an NNS/LYG of 9.1.
The NNS based on CISNET modeling results is much smaller than the NNI based on RCT data. Eighty-four women need to be screened annually between 40 and 84 years to save one life from breast cancer and 5.3 need to be screened annually to gain 1 life-year from breast cancer.
R. Edward Hendrick1 Mark A. Helvie2
DOI:10.2214/AJR.11.7146 Received May 2, 2011; accepted after revision August 30, 2011. R. E. Hendrick is a consultant for GE Healthcare on digital breast tomosynthesis and serves on the medical advisory boards for GE Healthcare, Koning Corp., and Bracco. M. A. Helvie receives grant funding from GE Healthcare through the University of Michigan. None of this work has been shared with a commercial party.
Department of Radiology, University of Colorado–Denver, School of Medicine, 12700 E 19th Ave, Mail Stop C278, Aurora, CO 80045. Address correspondence to R. E. Hendrick ([email protected])
Department of Radiology, Breast Imaging Section, University of Michigan Health System, Ann Arbor, MI.
AJR 2012; 198:723–728
0361–803X/12/1983–723
American Roentgen Ray Society
AJR:198, March 2012.
With screening, breast cancer deaths were reduced by 48% for women 40– 49 years old, which was similar to the 44% reduction for women 40–69 years old. Coldman et al. [26] documented the outcomes of over 2.7 million women in seven provincial service screening programs that served 85% of Canadian women; from 1990 to 2009, mortality reduction among screened women was 44% for women 40–49 years old, which was similar to the 40%, 42%, and 35% reductions for women 50–59, 60–69, and 70– 79 years old, respectively. An observational study from the Breast Cancer Surveillance Consortium (BCSC), a National Cancer Institute–sponsored longitudinal study involving seven regions of the United States, found that tumors in women 45–49 years old behaved similarly to those in women 50–59 years old and concluded that these groups of women should be screened similarly [27]. Finally, Hellquist et al. [28] reported on service screening in Sweden for women 40– 49 years old from 1986 to 2005. After a median 16-year follow-up, breast cancer mortality rates were 26% lower in counties that invited women to screening than in those that did not. Because treatments available to women with breast cancer were the same across Sweden through the nationalized health system, the observed differences in mortality were due to screening alone. In summary, because observational studies of service screening mammography reflect actual clinical practice, more current practice, and larger populations, they overcome some limitations of RCTs. Observational studies have found much greater mortality reductions for women 40–49 years old than RCTs have. Additionally, observational studies have found mortality reductions for women in this age group that were similar to those for older women [26, 29, 30]. Although observational studies are subject to selection bias, the bias does not account for the very large difference in mortality reduction between observational studies and RCTs.
The burden of breast cancer among women 40–49 years old is substantial, particularly when life-years lost without screening are taken into account. A large body of evidence shows that annual screening mammography beginning at 40 years old results in the greatest mortality benefit and the most life-years gained. Efforts to limit screening to women 40–49 years old who have elevated risk would miss the great majority of detectable breast cancers. As screening technology continues to improve, the balance of benefits versus risks is expected to further shift in favor of screening women 40–49 years old.
Kimberly M. Ray1 Bonnie N. Joe1 Rita I. Freimanis1 Edward A. Sickles1 R. Edward Hendrick2
doi.org/10.2214/AJR.17.18707 Received July 1, 2017; accepted after revision September 5, 2017. R. E. Hendrick is a consultant to GE Healthcare on work unrelated to this manuscript.
R. E. Hendrick is a consultant to GE Healthcare on work unrelated to this manuscript
1 Department of Radiology and Biomedical Imaging, University of California, San Francisco, 1600 Divisadero St, Box 1667, C-250, San Francisco, CA 94115. Address correspondence to B. N. Joe ([email protected]). 2 Department of Radiology, University of Colorado School of Medicine, Aurora, CO. Women’s Imaging • Review AJR 2018; 210:264–270 0361–803X/18/2102–264 © American Roentgen Ray Society.
IMPORTANCE: Breast cancer is a leading cause of premature mortality among US women. Early detection has been shown to be associated with reduced breast cancer morbidity and mortality. OBJECTIVE To update the American Cancer Society (ACS) 2003 breast cancer screening guideline for women at average risk for breast cancer.
PROCESS: The ACS commissioned a systematic evidence review of the breast cancer screening literature to inform the update and a supplemental analysis of mammography registry data to address questions related to the screening interval. Formulation of recommendations was based on the quality of the evidence and judgment (incorporating values and preferences) about the balance of benefits and harms.
EVIDENCE SYNTHESIS: Screening mammography in women aged 40 to 69 years is associated with a reduction in breast cancer deaths across a range of study designs, and inferential evidence supports breast cancer screening for women 70 years and older who are in good health. Estimates of the cumulative lifetime risk of false-positive examination results are greater if screening begins at younger ages because of the greater number of mammograms, as well as the higher recall rate in younger women. The quality of the evidence for overdiagnosis is not sufficient to estimate a lifetime risk with confidence. Analysis examining the screening interval demonstrates more favorable tumor characteristics when premenopausal women are screened annually vs biennially. Evidence does not support routine clinical breast examination as a screening method for women at average risk.
RECOMMENDATIONS: The ACS recommends that women with an average risk of breast cancer should undergo regular screening mammography starting at age 45 years (strong recommendation). Women aged 45 to 54 years should be screened annually (qualified recommendation). Women 55 years and older should transition to biennial screening or have the opportunity to continue screening annually (qualified recommendation). Women should have the opportunity to begin annual screening between the ages of 40 and 44 years (qualified recommendation). Women should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer (qualified recommendation). The ACS does not recommend clinical breast examination for breast cancer screening among average-risk women at any age (qualified recommendation).
CONCLUSIONS AND RELEVANCE: These updated ACS guidelines provide evidence-based recommendations for breast cancer screening for women at average risk of breast cancer. These recommendations should be considered by physicians and women in discussions about breast cancer screening.
Kevin C. Oeffinger, MD; Elizabeth T. H. Fontham, MPH, DrPH; Ruth Etzioni, PhD; Abbe Herzig, PhD; James S. Michaelson, PhD; Ya-Chen Tina Shih, PhD; Louise C. Walter, MD; Timothy R. Church, PhD; Christopher R. Flowers, MD, MS; Samuel J. LaMonte, MD; Andrew M. D. Wolf, MD; Carol DeSantis, MPH; Joannie Lortet-Tieulent, MSc; Kimberly Andrews; Deana Manassaram-Baptiste, PhD; Debbie Saslow, PhD; Robert A. Smith, PhD; Otis W. Brawley, MD; Richard Wender, MD.
JAMA. 2015;314(15):1599-1614. doi:10.1001/jama.2015.12783 Corrected on April 5, 2016.